Your cart is currently empty!
Food allergy prevention is now a core part of infant feeding guidance, and the American Academy of Pediatrics (AAP) has moved away from delayed introduction of allergens toward “early, purposeful” exposure for most babies. This article walks you through, in a professional, pediatric‑friendly way, which allergens to start, when, and how—fully aligned with current AAP‑style recommendations and complementary global guidelines.
In this guide you’ll learn:
- Which allergens to focus on.
- When to start them (around 6 months, not 1–3 years).
- How to introduce them in safe, easy‑to‑digest forms.
This article explains, in simple, practical terms, which allergens to start, when to start them, and how to introduce them safely between 6–12 months, all in line with current AAP‑style guidance.
Why Early Introduction Now?
For many years, AAP‑associated guidelines suggested delaying allergenic foods; that stance has been replaced by evidence‑based early introduction in the first year of life. Landmark studies showed that early and regular peanut intake can reduce peanut allergy risk by up to 80% in high‑risk infants.
Current AAP guidance now emphasizes:
- No routine delay of common allergens (egg, peanut, cow’s milk, tree nuts, wheat, soy, fish, shellfish).
- Early introduction as part of complementary feeding, usually around 6 months of age, when solid foods begin.
- Regular, ongoing feeding (at least weekly) once an allergen is safely introduced.
Key Allergens & Recommended Timing
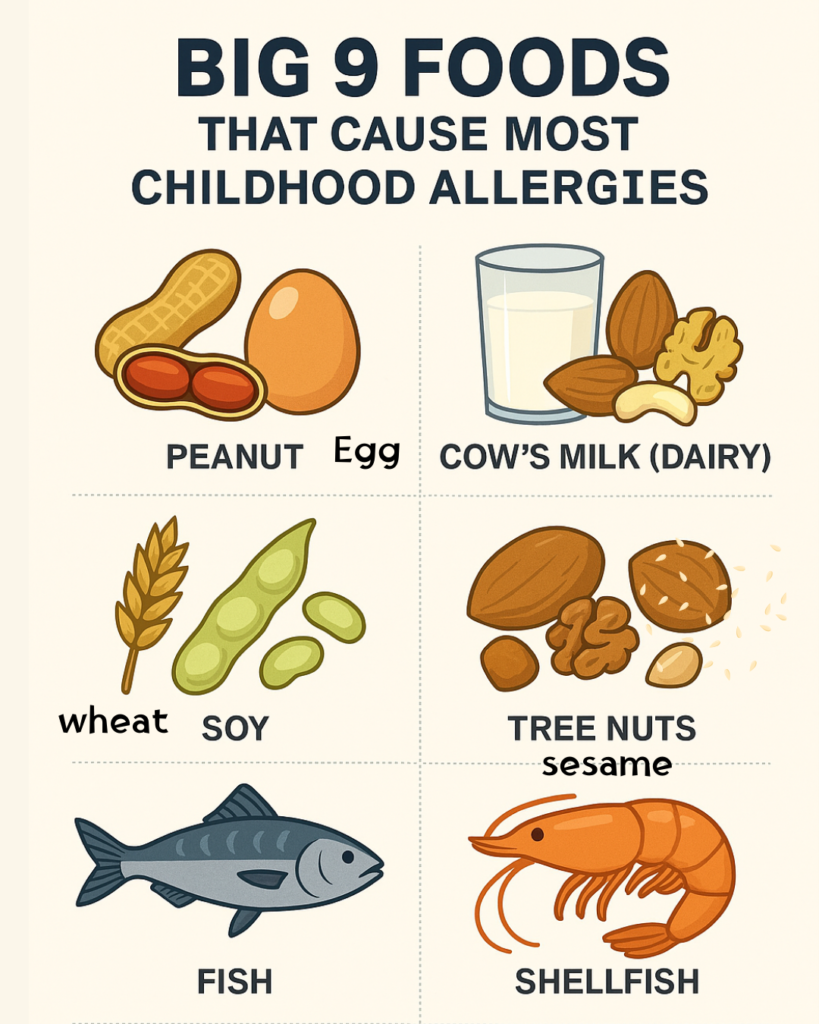
The AAP and AAP‑referenced guidelines focus on the “Big 9” allergens as priority targets for early introduction:
Peanut
Egg
Cow’s milk (dairy)
Tree nuts (e.g., almonds, walnuts, cashews)
Wheat
Soy
Fish (e.g., salmon, cod)
Shellfish (e.g., shrimp, crab)
Sesame (increasingly recognized as a major allergen)
You do not need to introduce all of these on day 1. The goal is to gradually add them into your baby’s diet, starting around 6 months, in safe, easy‑to‑digest forms.
Peanut
- AAP‑endorsed expert panels recommend introducing peanut between 4–6 months of age for all infants, if they are developmentally ready for solids and have no contraindications.
- For high‑risk infants (severe eczema and/or egg allergy), evaluation by a pediatrician or allergist may be advised before home introduction, and peanut may be started under medical supervision.
Egg
- AAP‑aligned data now support introducing well‑cooked egg around 6 months alongside other solids.
- High‑risk infants (severe eczema or other food allergies) may benefit from clinician guidance but still should not avoid egg; early introduction is preferred over delay.
Cow’s Milk (dairy)
- Whole cow’s milk as a drink is still not recommended before 12 months because it can cause iron deficiency and GI issues.
- However, cow’s‑milk proteins in cooked form (yogurt, cheese, milk‑based porridge) can be introduced as part of solids from around 6 months, provided there is no clear allergy history.
Tree nuts, wheat, soy, fish, shellfish, sesame
- AAP‑referenced guidelines state these can be introduced when other complementary foods are introduced, typically around 6 months, in age‑appropriate, safe forms.
- For high‑risk infants, consultation with the pediatrician or allergist is reasonable but avoidance is no longer recommended as a preventive strategy.
When to Start?
AAP‑linked feeding guidance ties allergen introduction to developmental readiness for solids, not a strict calendar age.
Low‑risk infants (no eczema, no known allergy)
- Start allergens around 6 months, once baby:
- Has good head control.
- Can sit with support.
- Shows interest in food.
- Begin with one allergen at a time, every day or every other day, then gradually add another after 2–3 days.
High‑risk infants (severe eczema and/or existing food allergy)
- AAP‑endorsed addendum guidelines recommend evaluating peanut risk and, for many high‑risk babies, introducing peanut between 4–6 months, often under clinician guidance.
- This population may benefit from:
- Review of skin‑prick or specific‑IgE testing.
- Possible supervised in‑office introduction for peanut or egg.
How to Introduce Allergens Safely?
AAP‑referenced guidance stresses safety, frequency, and observation, not perfection.
General AAP‑aligned strategy:
- Start small: Begin with a very small amount (e.g., 1/4 to 1/2 teaspoon of peanut butter thinned in breast milk/formula or water).
- Serve it at home, early in the day: So you can monitor for 2–4 hours and seek care if needed.
- Watch for signs of reaction:
- Mild: facial or perioral rash, mild hives away from lips.
- Severe: difficulty breathing, wheezing, vomiting, swelling of lips/tongue, lethargy—call 911/seek emergency care immediately.
Red Flags & When to Stop or Seek Help:
AAP‑linked and global allergy‑prevention guidelines emphasize that mild reactions are not a reason to indefinitely avoid a food, but severe reactions require medical management.
- If you see any of the following, stop feeding and seek urgent evaluation:
- Trouble breathing, wheezing, noisy breathing.
- Swelling of lips, tongue, or face.
- Persistent vomiting, diarrhea, or lethargy after eating.
- Sudden paleness or collapse.
- If your baby has a history of severe reactions or multiple allergies, coordinate with a pediatric allergist on a personalized reintroduction plan.
How to Introduce Each Allergen Safely
AAP‑referenced guidelines emphasize safety, frequency, and observation, not perfection. Here’s how to introduce each major allergen in a way that fits solid‑food guidelines and avoids choking hazards.
Peanut:
- Form: Thin peanut butter mixed into baby‑friendly foods (pureed vegetables, porridge, yogurt) or use a commercial peanut‑allergen powder designed for babies.
- Methods:
- Mix ½–1 teaspoon of peanut butter with breast milk, formula, or warm water to make a smooth paste, then swirl it into a puree.
- Alternatively, mix it into a soft fruit mash (banana, avocado).
- Avoid: Whole peanuts, thick globs of peanut butter, or unthinned spreads that can block the airway.
- When to start: Around 6 months for low‑risk babies; 4–6 months for many high‑risk babies, under clinician advice.
- Frequency: Once tolerated, aim to give 2 grams of peanut protein at least 3 times per week or at least weekly, as long‑term studies show this helps maintain tolerance.
Egg:
- Form: Well‑cooked egg (hard‑boiled and mashed, scrambled, or finely chopped) mixed into mashed vegetables, porridge, or pasta.
- Safety: Avoid runny or raw eggs; always cook until the yolk and white are firm.
- When to start: Around 6 months, once your baby is eating other solids.
- Frequency: After safe introduction, include egg in meals 1–2 times per week or more, depending on tolerance and family eating habits.
Cow’s Milk (Dairy):
- Important: Whole cow’s milk as a drink is not recommended before 12 months because it can cause iron deficiency and gastrointestinal issues.
- Safe forms for babies:
- Yogurt (plain or lightly sweetened, with no added honey).
- Cheese (soft, grated, or melted into veggies or pasta).
- Milk‑based porridge (cows’ milk mixed into oatmeal or other grain‑based cereals).
- When to start: Around 6 months, once your baby is eating solids, provided there is no clear allergy history.
- Frequency: If tolerated, include dairy‑based meals 2–4 times per week as part of varied complementary feeding.
Tree Nuts, Wheat, Soy, Fish, Shellfish, Sesame:
AAP‑referenced guidelines state that these foods can be introduced when your baby is developmentally ready for solids, typically around 6 months, in safe, age‑appropriate forms.
- Tree nuts: Avoid whole nuts and large chunks. Use nut butters thinly spread on toast or mixed into purees, or purchase baby‑specific nut‑butter blends.
- Wheat: Offer soft cooked pasta, bread, or wheat‑based cereals that are easy to mash or gum.
- Soy: Include tofu, soy‑based cereals, or soy‑based yogurt in small amounts, mixed with vegetables or grains.
- Fish and shellfish: Use well‑cooked, bone‑free, flaked fish or finely chopped shellfish mixed into mashed vegetables or rice.
- Sesame: Use sesame paste (tahini) thinned in warm water or yogurt, avoiding whole sesame seeds while your baby is still young.
For high‑risk infants, AAP‑style guidance still does not recommend routine avoidance; instead, many allergists prefer early, supervised introduction.
How Often Should You Give Allergens?
The new mantra in allergy prevention is: “Eat Early. Eat Often”
Once a food is safely introduced and your baby shows no reaction:
- Offer that food at least once per week, and ideally more often.
- This repeated exposure helps teach the immune system that the food is safe and reduces the risk of developing an allergy over time.
You do not need to give every allergen every day. The goal is regular, ongoing inclusion in your baby’s diet, not perfection.
What Does a Reaction Look Like?
AAP‑linked allergy and pediatric‑nutrition resources stress knowing the difference between mild, moderate, and severe reactions.
Mild reactions
These may be uncomfortable but are usually not life‑threatening and can still be medically evaluated. Signs include:
- A small rash or redness around the mouth or on the face.
- Mild hives that appear and fade quickly.
- Mild fussiness or mild spitting up.
Even with mild reactions, stop feeding that food at that meal and call your pediatrician for advice.
Severe (emergency) reactions
These are medical emergencies and require immediate medical care (call 911 or go to the ER). Signs include:
- Difficulty breathing, wheezing, or noisy breathing.
- Swelling of the lips, tongue, or face.
- Persistent vomiting, diarrhea, or abdominal pain after eating.
- Lethargy, paleness, or collapse.
If your baby has a severe reaction, do not try home remedies or herbal treatments. Seek emergency care immediately and follow your doctor’s plan for future feeding.
Leave a Reply
You must be logged in to post a comment.